PART 2: “STOP RESISTING!” While He’s Literally Having a Stroke — Fredericksburg Police Brutality Caught on Bodycam Sparks Outrage!c
PART 2: “STOP RESISTING!” While He’s Literally Having a Stroke — Fredericksburg Police Brutality Caught on Bodycam Sparks Outrage!
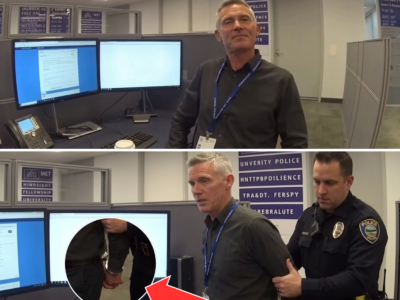
The Fredericksburg incident involving David Washington has become a case study in systemic failure across law enforcement and emergency medical response. Washington, a 34-year-old man suffering a stroke while driving erratically, was treated as a criminal suspect rather than a patient in urgent medical distress. This deadly misinterpretation underscores the urgent need for nationwide reforms in training, accountability, and crisis management.
Mental Health and Medical Crisis Training:
One of the most critical takeaways from this case is the necessity for comprehensive crisis intervention training. Officers are now being instructed to recognize medical emergencies — including strokes, hypoglycemia, seizures, and psychiatric episodes — as scenarios requiring immediate medical assessment before any use of force. Departments nationwide are integrating simulated medical crisis scenarios into routine academy training, teaching officers to differentiate between deliberate resistance and symptoms of medical or mental health crises.
De-escalation Protocols:
Fredericksburg’s officers defaulted to force escalation rather than assessment. As a result, nationwide police training programs are emphasizing de-escalation as a core skill. Officers are instructed to maintain safe distances, employ verbal communication first, and involve medical professionals whenever possible. Non-lethal measures, including restraint alternatives and controlled containment strategies, are now central to preventing fatalities during ambiguous encounters.
EMS Integration and Accountability:
The David Washington case highlights gaps in coordination between police and EMS personnel. Following the incident, EMS agencies have revised protocols requiring immediate assessment and intervention, even when law enforcement is present. Paramedics are empowered to override non-essential police commands to prioritize life-saving measures, ensuring that medically vulnerable individuals are stabilized before further enforcement actions. Federal guidance encourages joint training exercises to synchronize police and medical response during emergencies.
Civilian Oversight and Transparency:
To prevent recurrence of similar tragedies, Fredericksburg and other municipalities have established independent civilian oversight boards empowered to review excessive force incidents, evaluate officer compliance, and recommend disciplinary action. These boards enhance accountability and provide community involvement, ensuring that systemic patterns of negligence or misuse of authority are corrected proactively rather than reactively.

Bodycam and Digital Evidence Policies:
Bodycam footage from the Washington encounter was pivotal in establishing the facts. Nationwide, law enforcement agencies are now required to maintain strict activation protocols for bodycams, with footage stored securely and reviewed in cases involving medical or psychiatric emergencies. This ensures objective documentation, supports civil and criminal investigations, and provides critical evidence for training and policy development.
Legal Implications and Qualified Immunity:
The Fredericksburg case challenges traditional interpretations of qualified immunity. Officers can no longer assume blanket protection when misinterpreting medical emergencies as resistance. Civil rights litigation stemming from incidents like Washington’s stroke now emphasizes the importance of timely assessment and proportional response. Federal appellate rulings reinforce that failure to intervene or recognize medical distress constitutes a violation of constitutional rights, holding officers and departments accountable for preventable injuries or deaths.
Policy Implementation Across States:
Following the case, multiple states have issued directives for standardized crisis management. These include mandatory medical emergency recognition, mental health intervention protocols, and clear documentation standards for all first responders. Departments in North Carolina, California, and Texas are using the Washington incident as a training benchmark, demonstrating both the consequences of inaction and the life-saving potential of properly executed protocols.
Community Engagement and Public Trust:
The incident has had a profound impact on public perception of policing. Trust is restored not only through legal accountability but through proactive communication and transparency. Town halls, community review boards, and public reporting mechanisms allow citizens to observe the implementation of new protocols, ensuring that reforms are enforced consistently and that families have confidence in emergency response systems.
Financial and Systemic Accountability:
Civil settlements related to medical emergencies like Washington’s highlight the fiscal consequences of systemic failure. Municipalities face millions in compensation when officers fail to recognize and respond appropriately to medical crises. This financial exposure incentivizes departments to adopt rigorous training, oversight, and procedural reforms, aligning policy with both public safety and fiscal responsibility.
Cultural Shifts in Policing:
The case illustrates the urgent need to shift departmental culture from enforcement-first to care-first. Officers must view civilians through a lens that prioritizes life and safety while balancing law enforcement responsibilities. Organizational change includes reassessing recruitment, training, and supervision to ensure officers understand the profound risks of misinterpreting medical emergencies.
Long-Term Lessons:
David Washington’s ordeal demonstrates that even brief delays or misjudgments during a medical crisis can be fatal. Nationwide, the incident serves as a cautionary tale about the interplay between medical understanding, crisis management, and law enforcement authority. Departments are now embedding cross-disciplinary approaches, integrating police, EMS, and mental health professionals to mitigate risk and ensure every encounter prioritizes human life.
In conclusion, the Fredericksburg stroke case underscores the deadly consequences of systemic negligence, inadequate training, and mismanaged crisis response. DOJ guidance, state mandates, and municipal reforms now emphasize crisis intervention, bodycam transparency, civilian oversight, and life-preserving de-escalation. Officers nationwide are learning that failure to recognize medical emergencies is not only ethically indefensible but legally perilous.
News

SHOCKWAVE BROADCAST: Viral Street Footage Showing Religious Clashes, Political Tension, and Extreme Claims Leaves Viewers Divided Worldwide
SHOCKWAVE BROADCAST: Viral Street Footage Showing Religious Clashes, Political Tension, and Extreme Claims Leaves Viewers Divided Worldwide A newly circulated compilation of street interviews and public confrontations filmed in Western…

THE INTERVIEW THAT TORCHED THE ROOM: Reporter Left Frozen After Imam Says Secular Law Can “Go to Hell”
THE INTERVIEW THAT TORCHED THE ROOM: Reporter Left Frozen After Imam Says Secular Law Can “Go to Hell” The room did not explode all at once. It tightened first. A…

THE STREET SPEECH THAT SET BRITAIN ON FIRE: A PATRIOT’S PROVOCATIVE WORDS SPARK CHAOS, POLICE ACTION, AND A FREE-SPEECH WAR
THE STREET SPEECH THAT SET BRITAIN ON FIRE: A PATRIOT’S PROVOCATIVE WORDS SPARK CHAOS, POLICE ACTION, AND A FREE-SPEECH WAR A tense street confrontation in Britain has erupted into a…

“BRITAIN IN CHAOS? Belfast Riots EXPLODE After Knife Attack — Immigration, Violence, and Political Firestorm Rock the UK”
“BRITAIN IN CHAOS? Belfast Riots EXPLODE After Knife Attack — Immigration, Violence, and Political Firestorm Rock the UK” A wave of unrest in Northern Ireland has escalated into one of…

“EXPOSED! Pakistani Woman Who Harassed Jews in Vietnam Gets HUMILIATED by British Police Investigation After Viral Hate Video EXPLODES Online”
“EXPOSED! Pakistani Woman Who Harassed Jews in Vietnam Gets HUMILIATED by British Police Investigation After Viral Hate Video EXPLODES Online” A viral confrontation involving two Israeli tourists in Vietnam has…

PART 2: A Waitress Was Accused of Stealing $57,000 — Then a Detective Ignored the Law and Turned an Interview Into a Case That Could Collapse in Court
PART 2: A Waitress Was Accused of Stealing $57,000 — Then a Detective Ignored the Law and Turned an Interview Into a Case That Could Collapse in Court After the…
End of content
No more pages to load