The Silent Crisis in Your Colon: Understanding Diverticulosis and Diverticulitis
The Silent Crisis in Your Colon: Understanding Diverticulosis and Diverticulitis
It begins almost imperceptibly, often decades before the first sharp pang of agony signals that something is wrong. In the quiet corridors of the digestive tract, small, marble-sized pouches begin to bulge outward through weak spots in the colon wall. This condition, known as diverticulosis, is one of the most common—and most misunderstood—gastrointestinal ailments in the modern world.
For millions of Americans, these pouches remain a silent, lifelong companion, discovered only incidentally during a routine screening. But for a significant minority, this “silent” condition can erupt into a medical emergency. Understanding the difference between the presence of these pouches (diverticulosis) and the often-painful inflammation or infection that can follow (diverticulitis) is not just a matter of clinical terminology—it is a vital component of digestive health and long-term wellness.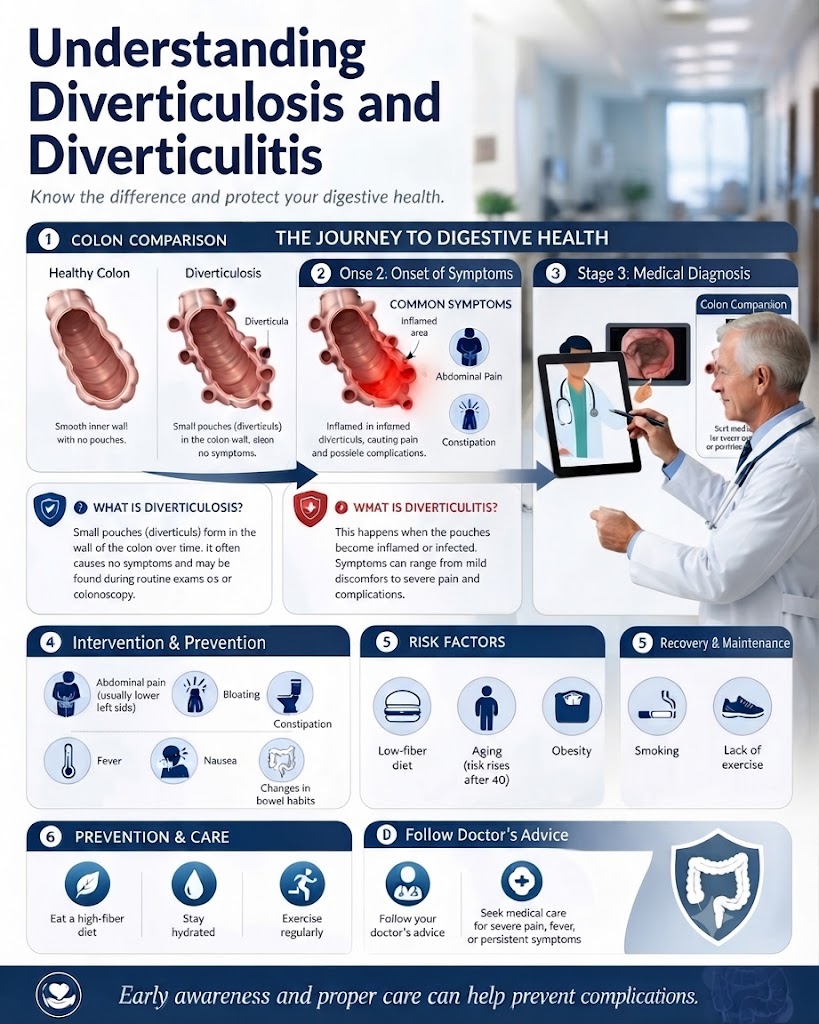
What Are Diverticula and Why Do They Form?
To understand diverticular disease, one must first visualize the colon not as a static tube, but as a muscular organ that contracts to push waste toward the exit. In an ideal digestive environment, these contractions are smooth and efficient. However, in the modern American diet, which is frequently defined by high-sugar, high-fat, and low-fiber intake, the process often hits a snag.
When fiber is scarce, stool becomes hard and difficult to pass. This forces the colon to exert significantly more pressure to move the waste forward. Think of the colon wall like a tire; if there are weak spots, persistent internal pressure will eventually cause a “blowout”—or in this case, a protrusion. These small herniations pushing outward through the muscular wall are called diverticula.
While their formation is essentially a structural response to chronic pressure, they are not inherently dangerous. In fact, most people who have them are completely asymptomatic. However, their presence changes the landscape of the colon, creating potential traps for bacteria and digestive waste.
The Critical Distinction: Diverticulosis vs. Diverticulitis
It is common for patients to use these terms interchangeably, but they represent two vastly different clinical stages.
Diverticulosis is the baseline condition: the mere presence of diverticula in the colon. It is usually a chronic, non-inflammatory state. Most patients do not require treatment, and many will never know they have it until a colonoscopy reveals the “pockets” lining their intestines.
Diverticulitis, conversely, is an acute medical event. It occurs when one or more of these pouches becomes inflamed or infected—often because stool or bacteria have become trapped inside the sac, leading to irritation, swelling, and potential rupture. While diverticulosis is a “condition,” diverticulitis is a “disease” that can range from a manageable outpatient nuisance to a life-threatening emergency requiring surgical intervention.
The American Lifestyle: Identifying the Risk Factors
The rise of diverticular disease in the West is not a coincidence; it is a byproduct of our lifestyle. While genetics play a role—some people are simply born with weaker colon walls—environmental factors are the primary drivers of this epidemic.
The Fiber Gap
The single greatest risk factor for diverticular disease is a lack of dietary fiber. Fiber acts as the “ballast” of our digestive system, adding bulk to stool and ensuring it moves through the colon with minimal resistance. When we swap whole grains and vegetables for processed snacks, we inadvertently turn our colon into a pressure cooker.
The Aging Process
Time is the great equalizer of the digestive tract. The risk of developing diverticula increases significantly after age 40 and accelerates after age 60. As the tissues of the colon lose their elasticity, they become more prone to herniation.
Lifestyle Choices
Obesity: A higher Body Mass Index (BMI) is associated with increased pressure on the colon and a higher likelihood of complicated disease.
Physical Inactivity: Regular exercise promotes bowel motility; sedentary behavior is a known enemy of gut health.
Tobacco Use: Smoking has been definitively linked to more severe, complicated episodes of diverticulitis.
Medication Side Effects: Chronic use of non-steroidal anti-inflammatory drugs (NSAIDs) like ibuprofen or naproxen, as well as steroids and certain opioids, can interfere with the mucosal lining of the gut and exacerbate inflammation.
Recognizing the Warning Signs
Because diverticulitis can escalate rapidly, knowing when to seek help is critical. The classic presentation involves a sudden, persistent ache, most commonly in the lower left quadrant of the abdomen—the location of the sigmoid colon.
Common Symptoms:
Localized Pain: A tenderness that often feels like a “left-sided appendicitis.”
Systemic Distress: Fever, chills, and nausea.
Bowel Changes: Unexplained constipation or, conversely, diarrhea.
Abdominal Bloating: A feeling of fullness or trapped gas that does not resolve.
When to Seek Emergency Care:
Do not wait for a primary care appointment if you experience:
Severe, debilitating abdominal pain that makes it difficult to stand.
High fever accompanied by shaking chills.
Visible blood in the stool.
Persistent vomiting that prevents you from keeping fluids down.
Tachycardia (racing heart rate), which can indicate an internal infection or sepsis.
The Path to Complications: Why Treatment Matters
When left unaddressed, or when an acute attack is severe, diverticulitis can lead to a cascade of complications that move from the digestive tract into the abdominal cavity.
Abscesses: A walled-off pocket of pus forms around the infected diverticulum, requiring antibiotics or drainage.
Perforation: The inflamed pouch may develop a micro-perforation, leaking bacteria into the abdominal cavity.
Peritonitis: This is the “worst-case scenario”—the leakage of infected material causes inflammation of the abdominal lining, a life-threatening condition.
Obstruction: Chronic inflammation can cause scarring, narrowing the colon and physically blocking the passage of stool.
Fistulas: An abnormal tunnel forms between the colon and other organs, such as the bladder or vagina, leading to recurring infections.
Diagnostic Standards and Treatment Strategies
If you suspect a flare-up, your doctor will likely move quickly. The “gold standard” for diagnosing diverticulitis is a CT scan of the abdomen. This imaging allows physicians to see not only the diverticula but also the presence of gas, fluid, or abscesses outside the colon, helping them grade the severity of the infection.
Managing the Flare-up
Treatment is highly personalized based on the severity:
Mild Cases: Often managed at home with a liquid diet, bowel rest, and sometimes a course of oral antibiotics. (Interestingly, recent research suggests that some very mild cases may not even require antibiotics, moving toward a “watch and wait” approach under medical supervision).
Moderate Cases: May require hospitalization for IV antibiotics, fluids, and pain management to ensure the bowel can rest.
Severe Cases: When perforation or abscesses occur, surgery may be necessary. This often involves a resection, where the diseased portion of the colon is removed, and the remaining ends are reconnected. In emergency situations, a temporary or permanent ostomy may be required.
The Future of Gut Health: Diet and Prevention
For those who have been diagnosed with diverticulosis, the focus should shift entirely toward prevention. The good news is that for the vast majority, the condition is manageable through lifestyle modifications.
Debunking the Old Myths
For decades, doctors told patients to avoid nuts, seeds, and popcorn, fearing these fragments would get stuck in the diverticula. Modern science has debunked this. Extensive studies have shown that these foods do not increase the risk of diverticulitis. In fact, many are high in fiber, which is precisely what the colon needs.
Building a “Diverticulosis-Friendly” Diet
Focus on a high-fiber regimen (aiming for 25–35g per day):
Whole Grains: Oats, barley, quinoa, and brown rice.
Fruits and Vegetables: Apples with the skin, berries, broccoli, carrots, and leafy greens.
Legumes: Lentils, chickpeas, and black beans.
Hydration: Fiber needs water to do its job. Without adequate hydration, high fiber can actually make constipation worse.
Lifestyle as Medicine
Stay Active: Aerobic exercise encourages the rhythmic contractions of the bowel.
Weight Management: Reducing intra-abdominal pressure can significantly lower the risk of complications.
Quit Smoking: This is non-negotiable for anyone looking to reduce the risk of severe intestinal flare-ups.
Final Thoughts: Taking Control
Diverticular disease is a silent condition that reflects our broader struggle with modern nutrition and sedentary living. It is not, however, a life sentence. While the pouches themselves may never disappear, their impact on your life can be minimized through a proactive approach to diet and health.
The greatest tool you have is awareness. By recognizing the subtle signs of digestive distress and making a commitment to a high-fiber, active lifestyle, you can move from a position of vulnerability to one of control. If you are over 40, talk to your gastroenterologist about your gut health during your next checkup. You may have nothing to worry about, but in the world of digestive health, the quietest conditions are often the ones that benefit most from an early, informed conversation.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition.